When most of us think about type 2 diabetes, we think about several things: problems with blood sugar control, insulin sensitivity, difficulty in losing weight, struggling with exercise, etc… Most of us, however, rarely, if ever, think about an obscure term known as the disposition index.
It is so obscure, it doesn’t even have its own Wikipedia page!
While most of the things we think about regarding type 2 diabetes are part of the condition, the reality is they are just individual pieces of the same puzzle.
That one thing that encapsulates all of this is the disposition index.
Why Type 2 Diabetes Occurs
The typical progression from normal blood glucose control to type 2 diabetic goes something like this:
Over time, our insulin begins to lose sensitivity. This can be due to a number of factors but is typically the result of chronically elevated blood sugar (glucose) as a result of our diet. As our insulin loses sensitivity, our pancreas starts to secrete more insulin to deal with the elevated blood sugar. Somewhere during this progression, most people start gaining weight, typically when insulin first starts losing sensitivity.
Eventually, insulin struggles to reduce blood sugar so the pancreas secretes more insulin. At some point, our pancreas is unable to continue secreting more insulin. This is when people get diagnosed as type 2 diabetic. They go to the doctor, get a blood test and find their blood glucose is too high. They then go through an OGTT (Oral Glucose Tolerance Test) and get diagnosed as a type 2 diabetic because blood sugars are not reduced appropriately.
In the two paragraphs above, insulin and blood glucose were mentioned frequently. So it it understandable when these things are mentioned as part of the Type 2 Diabetes condition. Notice that we haven’t even mentioned disposition index.
There is a good reason for that because the disposition index encompasses something else we haven’t mentioned: the pancreatic beta cells.
Pancreatic Beta Cells and Insulin
Insulin is released from the pancreas; more specifically, it is released from the beta cells of the pancreas. When your blood sugar is under control and insulin sensitivity is high, everything functions normally.
You eat a meal or a snack, your blood sugar elevates, your pancreas senses this, the beta cells secrete insulin, insulin does its job by reducing blood sugar and then insulin goes back to normal levels.
This entire relationship can be described with a mathematical function in both normal blood glucose control and type 2 diabetics. This function is known as the disposition index. See figure below.
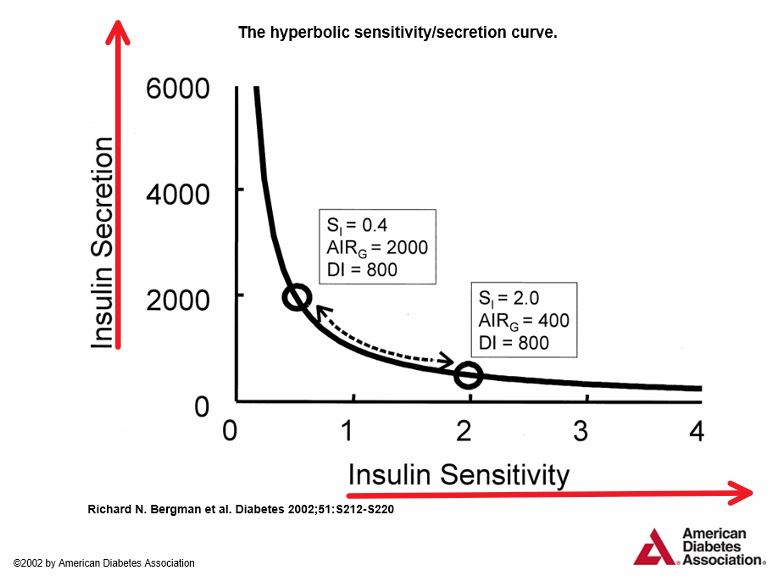
Source: Bergman et all, Diabetes, 2002, Figure 1, page S213.
Note: Red lines added.
The horizontal axis is insulin sensitivity and the vertical access is insulin secretion. What we can note from this figure is that as insulin sensitivity increases, insulin release decreases. We also note the opposite: As insulin sensitivity decreases, insulin release increases.
Based on research, we know the following: The work required by the pancreatic beta cells changes as insulin sensitivity changes – this can be seen by in the graph above by noting the increase in insulin release as we move left along the horizontal axis (insulin sensitivity).
As noted above (2nd italicized paragraph), at some point the pancreatic beta cells are unable to secrete more insulin in response to elevated blood sugar as insulin sensitivity decreases.
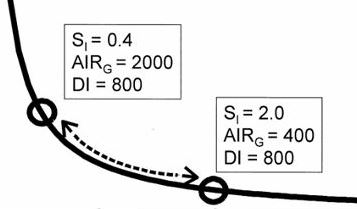
Note the two boxes in the graph above. We have zoomed in on them in the figure below. The two bottom numbers in the figure below in each of the boxes is 800 and represented by DI, which is the disposition index. So both have a disposition index of 800 but occupy different places on the function. How can this be?
The other numbers in the boxes give us the answer. “S” refers to insulin sensitivity and “AIR” refers to insulin release. The insulin release value in the left box is 2,000 pmol/l while it is 400 pmol/l in the right box. This means, for all practical purposes, that to achieve an optimal level of blood sugar control, when insulin sensitivity is 2.0 pmol/l (right box) we have to release 400 pmol/l of insulin. If insulin sensitivity decreases to 0.4 pmol/l, we have to release 2,000 pmol/l of insulin – a fivefold increase in insulin release.
What this means is that as insulin sensitivity decreases, the pancreatic beta cells have to do more work by secreting additional insulin to deal with the elevated blood sugar. The beta cells adapt to this additional work and over time, they reach an “insulin secretion limit.” This results in chronically elevated insulin and blood sugar, also known as type 2 diabetes.
But it is clear the dysfunction in pancreatic beta cells is the first domino to fall in this string of events.
So the main question is, what causes the beta cells to reach their limit? Why and/or how do they reach a point where they can no longer secrete insulin (or enough insulin)?
This is an active area of research, with new answers frequently. While there are answers to many questions, the precise mechanism has not been identified. And it may just be there are several factors that lead to this pancreatic beta cell dysfunction.
In our next post, we will cover some of the more promising areas of research. Included will be things you can do to increase the health of your pancreatic beta calls.
By implementing some of these suggestions, your insulin sensitivity will certainly change. This will also lead to an improvement in insulin release. Overall, this will lead to an improvement in your control of type 2 diabetes.
That’s something all of us want.

thank you very much!!! very helpful article.
Thank you. Glad you like it!